
Full disclosure. I did not learn these nuances about oscillometric blood pressure cuffs and mean arterial pressure (MAP) until I was a fellow in Critical Care Medicine. It is not widely taught. Do not feel bad that you did not know this. All I ask is for your help to share this with others so we all speak the same language and do the best for our patients.
We all do this every single day. We measure target many of our interventions in the critically ill patients to blood pressure. Whether it’s fluids, vasopressors, or blood pressure lowering agents, we obsess over these parameters. We feel warm and fuzzy if it’s okay. But are we using the right tool to find out these numbers?
What are the normal sounds when taking a blood pressure manually?
What are the normal sounds you hear with the “old fashioned”/auscultatory method of taking a patients blood pressure?
Those sounds define the systolic blood pressure and diastolic blood pressure respectively. Babadağ et al. has found that doing this method is extremely close to what one can find by using an arterial line.
Then you do math and could calculate the mean arterial pressure (MAP) by using the formula of (2xDBP)+SBP/3 but there are a number of different ways to derive the MAP. Does the BP cuff you have in the ICU, hospital or throughout the majority of doctor offices have ears? We if that’s the case, you CANNOT assume that the SBP and DBP provided by these devices are exact.
How do Oscillometric Devices Work?
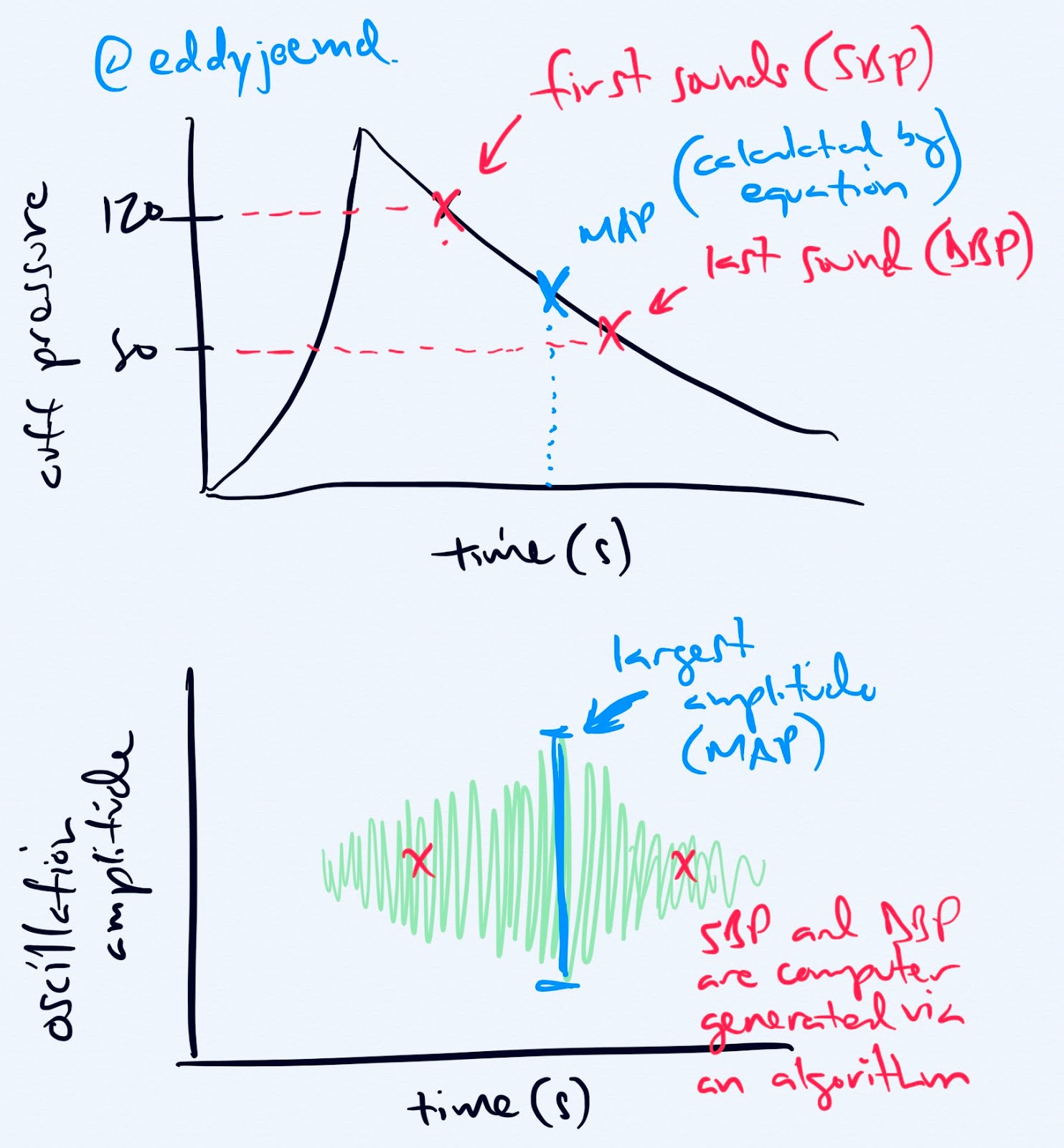
The device measures the oscillations from the blood vessel wall during cuff deflation. The maximal oscillation point is the MAP. The device uses an algorithm that is proprietary to define the SBP and DBP. Those algorithms are closely kept secrets to the manufacturers.
Why is this important, well, BP is GOLD in the ICU world. My nurses titrate pressors based on MAP number, as the guidelines suggest, but I have too often seen nurses whipping out their phone calculating the MAP by hand as they feel that the numbers generated on the screen are inaccurate. Now, this occurred when I trained in community academic hospital, then ivory tower fancy pants hospital, and now in a community hospital which is why I feel writing this post is so important. We need to understand how our technology works.
The MAP is the most important value generated by Oscillometric Devices
Per Yarrows et al. “the mean BP is determined at the peak of the amplitude of the oscillations”. This is the primary measurement. The SBP is assigned to be “approximately 55% prior to the maximum”. The DBP is “approximately 85% after the maximum oscillations”. They stress that the exact points are proprietary to each manufacturer. Liu et al. states “(MAP) is determined as the cuff pressure at which the maximum amplitude oscillation occurs. Systolic and diastolic pressures (SP and DP) are then determined as the cuff pressures at which the amplitude of cuff pressure oscillation is some ratio of its maximum value”. Those who think that the cuff directly measures SBP or DBP are just wrong.
In case you didn’t believe me with the first references, Sumlyan et al. states that “MBP, (is) a measurement made independently of the SBP and DBP”. In addition, they state that “mean blood pressure measurements and may offer the most reliable cuff estimate of the aortic pressure”. A third reference by Babbs states that “oscillometric method of measuring blood pressure with an automated cuff yields valid estimates of mean pressure but questionable estimates of systolic and diastolic pressures.”
Kiers et al. noted in a cohort study that compared calculated MAP vs. measured MAP. They found a significant difference between calculated MAP, i.e. the nurses/staff doing the calculation themselves, and the observed MAP (generated by the machine). They found that the generated MAP could either be lower or higher that the observed MAP. These differences were amplified even further when analyzed on individual patients rather than the cohorts. Would you feel comfortable treating your patients like this? I sure don’t. The conclusions state that “calculated and measured MAP cannot be used interchangeably”.
The authors discuss a trial where patients had their BP taken via oscillometric device in the OR vs. intraarterial and there was no statistically significant difference in the MAP. There was a difference in the SBP by 19mmHg, though. Could you imagine treating these patients based on an algorithm generated SBP? You’d be treating them (or not treating them) inappropriately!
What about Manual BP Measurements with MAP calculation vs. Arterial MAP?
Babadağ et al. looked at this question. They found that there was good correlation between manual BP measurements and measurements from the arterial line. It got muddy and inaccurate when the oscillometric devices came to play.
Why would an arterial line be beneficial over oscillometric technologies regarding the MAP?
I’ve always harped on arterial lines, although invasive, being the most reliable method of evaluating the blood pressure in our patients. If someone is critically ill on jet fuel, they’re getting an a-line. This is a fun study where they compared the oscillometric BP cuffs to a-lines in 736 patients by Kauffman et al.
When you look at the mean differences they obtained, the numbers weren’t too bad.
Systolic: 0.8mmHg
Diastolic: -2.9mmHg
Mean Arterial pressure: -1mmHg
This wouldn’t drive any of us crazy, right? We’d be cool with these differences if it avoids invasive (painful) interventions on our patients. But wait, there’s more. There was a large amount of variability which could lead to additional interventions.
Systolic: ± 15.7mmHg
Diastolic: ± 11mmHg
MAP: ± 10.2mmHg
The interesting part is that the ICU is a world of details and although the differences were small. The variation between the two, radial arterial line and oscillometric cuff, was enough though to cause additional treatment changes in more than 20% of patients. The article goes as far as to say that BP cuffs would not pass the Association for the Advancement of Medical Instrumentation standards. There’s no data as to how this changes outcomes.
This was a post hoc analysis (after the fact). This shouldn’t be too challenging to accomplish a prospective study looking at this in our critically ill patients. We have many patients who have a BP cuffs and an a-line in place. Why not just record cuff pressures every 15 minutes and obtain some data? Obviously it’s more complicated than that.
Wrapping up the MAP in Oscillometric Devices
Now, this post may seem like it’s being directed at nurses, after all, you all are the main ones at the bedside, but we all need to get better. The docs needs to stop presenting patients to each other by referencing the SBP. Docs need to stop telling nurses to hit SBP goals for their pressors instead of MAPs. If you use MAP to titrate vasopressors and want to learn more about vasopressors, CLICK HERE.
Well, now you know how this all works and you won’t make silly comments anymore. I hope I taught you something that in oscillometric devices you should trust the MAP.
Citations
Kiers HD, Hofstra JM, Wetzels JF. Oscillometric blood pressure measurements: differences between measured and calculated mean arterial pressure. Neth J Med. 2008 Dec;66(11):474-9. PMID: 19075313.
Link to Abstract
Link to FREE FULL PDF
Kaufmann T, Cox EGM, Wiersema R, Hiemstra B, Eck RJ, Koster G, Scheeren TWL, Keus F, Saugel B, van der Horst ICC; SICS Study Group. Non-invasive oscillometric versus invasive arterial blood pressure measurements in critically ill patients: A post hoc analysis of a prospective observational study. J Crit Care. 2020 Jun;57:118-123. doi: 10.1016/j.jcrc.2020.02.013. Epub 2020 Feb 22. PMID: 32109843.
Link to Article
Link to FULL FREE PDF
Yarows SA, Julius S, Pickering TG. Home blood pressure monitoring. Arch Intern Med. 2000 May 8;160(9):1251-7. doi: 10.1001/archinte.160.9.1251. PMID: 10809027.
Link to Article AND FULL FREE PDF
Smulyan H, Safar ME. Blood pressure measurement: retrospective and prospective views. Am J Hypertens. 2011 Jun;24(6):628-34. doi: 10.1038/ajh.2011.22. Epub 2011 Feb 24. PMID: 21350431.
Link to Article
Link to FULL FREE PDF
Babbs CF. Oscillometric measurement of systolic and diastolic blood pressures validated in a physiologic mathematical model. Biomed Eng Online. 2012 Aug 22;11:56. doi: 10.1186/1475-925X-11-56. PMID: 22913792; PMCID: PMC3541069.
Link to Article
Link to FULL FREE PDF
Liu J, Hahn JO, Mukkamala R. Error mechanisms of the oscillometric fixed-ratio blood pressure measurement method. Ann Biomed Eng. 2013 Mar;41(3):587-97. doi: 10.1007/s10439-012-0700-7. Epub 2012 Nov 21. PMID: 23180030.
Link to (NOT FREE) Article
Babadağ K, Zaybak A. Comparing Intra-Arterial, Auscultatory, and Oscillometric Measurement Methods for Arterial Blood Pressure. Florence Nightingale J Nurs. 2021 May 11;29(2):194-202. doi: 10.5152/FNJN.2021.19103. PMID: 34263238; PMCID: PMC8245021.
Link to Article
Link to FULL FREE PDF
Consider purchasing my book, ‘The Vasopressor & Inotrope Handbook’!

I have written “The Vasopressor & Inotrope Handbook: A Practical Guide for Healthcare Professionals,” a must-read for anyone caring for critically ill patients (check out the reviews)! You have several options to get a physical copy. If you’re in the US, you can order A SIGNED & PERSONALIZED COPY for $29.99 or via AMAZON for $32.99 (for orders in or outside the US).
Ebook versions are available via AMAZON KINDLE for $9.99, APPLE BOOKS, and GOOGLE PLAY.
¡Excelentes noticias! Mi libro ha sido traducido al español y está disponible a traves de AMAZON. Las versiones electrónicas están disponibles para su compra for solo $9.99 en AMAZON KINDLE, APPLE BOOKS y GOOGLE PLAY.
When you use these affiliate links, I earn an additional commission at no extra cost to you, which is a great way to support my work.
REELS SCRIPT
When your patients blood pressure cuff populates numbers on the screen, which one should you trust?
This is extremely important for you and your friends to understand as it could change the management of your patient.
I am creating this so you will stop manually calculating the MAP.
Please check out the links to read about this for yourself.
This is not medical advice.
When you take a manual blood pressure measurement, you listen for Korotkoff sounds.
Does the cuff in your hospitalized patient have ears? Nope.
That’s because our cuffs use oscillometric technology.
It measures the MAP and then populates the systolic and diastolic BP out of thin air from an algorithm.
It is not directly measuring systolic nor diastolic blood pressure.
So why would you go and work back ways to calculate a MAP?
Studies have shown that this calculated MAP is incorrect compared to the one on the monitor.
So please, trust the MAP on these devices above all else.
The systolic and diastolic pressures are questionable. Not the oscillometric map.
Disclaimer
Although great care has been taken to ensure that the information in this post is accurate, eddyjoemd, LLC shall not be held responsible or in any way liable for the continued accuracy of the information, or for any errors, omissions or inaccuracies, or for any consequences arising therefrom.